Associate Professor Details the Advances in Surgical Innovation in Ovarian Cancer

 Today marks the beginning of Ovarian Cancer Awareness Month, an important time to encourage discussion around a disease that an estimated 3,100 Canadian women will be diagnosed with in 2020. To help spread awareness, Associate Professor Dr. Taymaa May, has written a piece below about advances in surgical innovation surrounding Ovarian Cancer.
Today marks the beginning of Ovarian Cancer Awareness Month, an important time to encourage discussion around a disease that an estimated 3,100 Canadian women will be diagnosed with in 2020. To help spread awareness, Associate Professor Dr. Taymaa May, has written a piece below about advances in surgical innovation surrounding Ovarian Cancer.
Written by Dr. Taymaa May MD MSc FRCSC, Associate Professor with the Department of Obstetrics and Gynaecology at the University of Toronto.
Within gynaecologic oncology, epithelial ovarian cancer is the most challenging malignancy to treat. This carcinoma is often aggressive, with the majority of patients diagnosed with advanced stage disease, has high recurrence rates, and continues to be the leading cause of mortality from gynaecologic malignancies in Canada.
Patients with advanced ovarian cancer benefit from cytoreductive surgery - a major operative procedure that involves resection of all visible tumor in the abdomen and pelvis which may include removal of the gynaecologic structures, portions of the intestinal tract, liver, spleen and other intra-peritoneal structures. Comprehensive surgical cytoreduction has been shown to improve survival outcomes in women with advanced ovarian carcinoma. However, this complex surgical procedure carries a potential risk of perioperative morbidity. Significantly, most surgical complications lead to delays in recovery and delays in initiation of vital systemic therapy. This, in turn, may negatively impact long term survival. Timely surgical recovery is crucial to early introduction of systemic therapy in advanced ovarian malignancies, which is associated with improved progression-free and overall survival. Therefore, surgical expertise and surgical innovative techniques that minimize operative morbidity are key to improving overall outcomes in women with advanced ovarian cancers.
Our team conducted a surgical trial at the University Health Network/Sinai Health Systems (UHN/SHS), University of Toronto, examining the use of the fluorescent dye Indocyanine Green (ICG) and near-infra red camera technology, to assess anastomotic perfusion in patients undergoing bowel resection for gynaecologic malignancies. Ovarian malignancies are often metastatic at diagnosis and the tumor can involve portions of the intestine requiring segmental resection of the bowel. After reattaching the remaining bowel to reestablish the intestinal continuity, it is essential to ensure that the bowel anastomosis is well perfused. In the past, surgeons relied on visual inspection of the bowel and the tissues around it to determine tissue viability. ICG allows for precise assessment of mesenteric blood flow and bowel perfusion in real-time.
Our study documented our initial experience with the use of ICG for assessment of small and large bowel anastomoses in a series of 100 consecutive anastomoses performed by our team of gynaecologic oncology surgeons at UHN/SHS. Trans-anal and trans-abdominal near infra-red bowel perfusion assessment following ICG intra-vascular injection was safe, allowed for objective assessment of the bowel anastomoses and facilitated critical intra-operative decision-making [Figure].
I believe that integration of surgical innovation is integral to the growth and development of surgical programs such as the ovarian cancer gynaecologic oncology program. Our study on the use of ICG in the assessment of bowel viability following mutlivisceral tumor resection demonstrated favorable outcomes. As such, our group has integrated Indocyanine Green and near-infra red perfusion assessment as a standard of care technique for patients with gynaecologic malignancies undergoing bowel surgery. By optimizing surgical techniques and continuing to introduce and utilize surgically innovative tools, we can improve the surgical and oncologic outlook for women with ovarian malignancies.
FIGURE*
Transabdominal anastomotic perfusion assessment following small bowel resection and side-to-side reanastomosis for metastatic ovarian cancer using the SPY-PHI system (Striker, USA)
A: Transabdominal perfusion assessment showing well perfused bowel 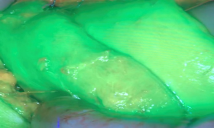 | B: Transabdominal perfusion assessment showing perfusion defect 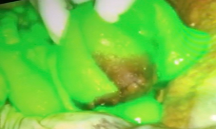 |
*Adapted from: Julie MV Nguyen, Liat Hogen, Stephane Laframboise, Genevieve Bouchard-Fortier, Sarah E Ferguson, Marcus Q Bernardini, Taymaa May. “The Use of Indocyanine Green Fluorescence Angiography to Assess Anastomotic Perfusion Following Bowel Resection in Multivisceral Surgery for Metastatic Gynecologic Malignancies- A Report of 100 Consecutive Anastomoses”. Gynecol Oncol. 2020 May 15:S0090-8258(20)31076-3.
_____________________________________________________________
Don't want to miss a post? Follow us on social media for more news!
FACEBOOK | INSTAGRAM | TWITTER
If you would like to be a guest blogger, please contact us at obgyn@utoronto.ca.